Proximal biceps injury
Biceps tendinitis / biceps tendinosis / biceps subluxation / biceps rupture
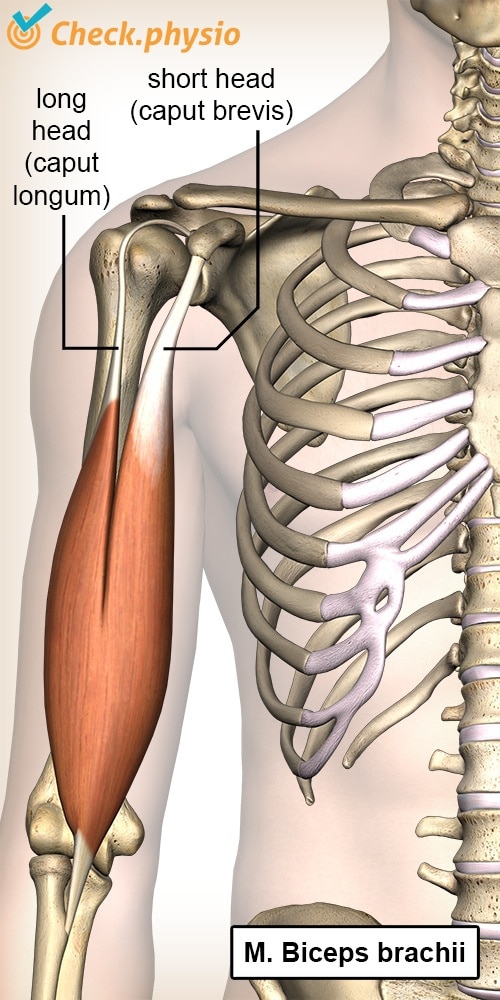
The biceps is the large muscle in the upper arm, the main function of which is to flex the elbow. It runs from the forearm over the front of the upper arm and into the shoulder. Biceps problems are often felt along the front of the shoulder and in the upper arm.
If the condition is located further down in the direction of the elbow, then this is referred to as a distal biceps injury.
Description of the condition
In the case of biceps tendinitis, the biceps tendon is inflamed. Tendinosis refers to decreased quality of the tendon (degeneration). This occurs with ageing or through inactivity.
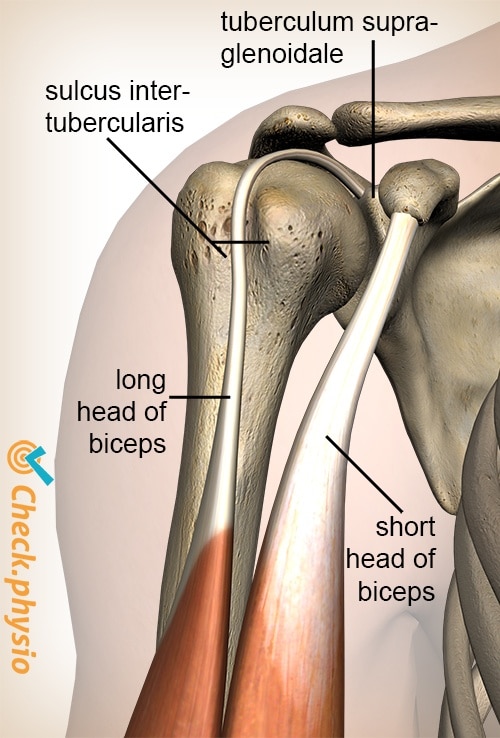
The long head of the biceps tendon runs along the front of the shoulder through a groove in the bone of the upper arm. We call this groof the 'sulcus intertubercularis' (bicipital groove). Tissue is stretched over the groove in order to keep the tendon in the groove and this forms a tunnel together with the bicipital groove. If this so-called 'transverse humeral ligament' tears, the biceps can move out of this groove and cause symptoms. This is referred to as a (sub)luxation of the biceps tendon.
In most cases of a rupture, the long head of the biceps tendon tears. The risk of a rupture increases with increasing degeneration of the tendon.
Cause and origin
Proximal biceps injuries often occur as a result of other shoulder injuries. The cause can therefore often be found in other disorders.
In five percent of the cases, a proximal biceps tendon injury occurs without any other shoulder injury. This includes acute trauma moments such as:
- Fall on a stretched arm.
- Excessive lifting.
- Overhand sport activities.
Signs & symptoms
Pain along the front of the shoulder that becomes worse with movements above shoulder height or when lifting heavy objects. The symptoms can sometimes be provoked by pressing on the biceps tendon on the front of the shoulder at the level of the bicipital groove (see image).
A subluxation may result in the above-mentioned symptoms, in addition to the patient regularly feeling something move along the front of the shoulder. The tendon of the long head of the biceps leaves the bicipital groove during movement. This can produce a snapping sound or sensation.
In the case of a rupture, the long head of the biceps tendon tears. The patient clearly feels something snap in the shoulder at the moment that a force is exerted on the tendon. This can occur during sports or when lifting a heavy object. A noticeable bump forms along the front inside of the upper arm. This is the long head of the muscle body of the biceps that has partially separated.
Diagnosis
By interviewing the patient about the complaints and a physical examination, a first diagnosis can be made. Because a proximal biceps injury is often a consequence of another shoulder disorder, the entire shoulder will be tested.
If instability or a rupture of the biceps tendon is suspected, imaging tests are necessary to reach the correct diagnosis. Unless a Popeye deformity is present, a rupture is the only possibility and additional testing is not necessary for this reason. However, in this case additional testing can be advised to check for any other shoulder injuries.
Additional testing can consist of X-rays, ultrasound or an MRI.
Treatment
Treatment depends on many factors.
Biceps tendinopathy (biceps tendinitis)
Biceps tendinopathy is treated conservatively (not surgically). Treatment consists mainly of physiotherapy and possibly painkillers or anti-inflammatory drugs. The physiotherapist has various treatment options for this. Because tendinopathy is caused by strain or other shoulder disorders, the emphasis is on repairing the tendon tissue. This requires 'relative' rest, movements that provoke the pain should be avoided. In addition, the treatment will mainly consist of optimizing the shoulder movement. This can be done by using
Exercises
You can check your symptoms using the online physiotherapy check or make an appointment with a physiotherapy practice in your area.
References
Catherine, A. & Churgay, M.D. (2009). Diagnosis and treatment of biceps tendinitis and tendinosis. Am Fam Physician. 2009;Sep 1;80(5):470-476.
Malik, S., Chiampas, G. & Leonard, H. (2010). Emergent evaluation of injuries to the shoulder, clavicle, and humerus. Emerg Med Clin N Am 2010;28:739-763.
Verhaar, J.A.N. & Linden, A.J. van der (2005). Orthopedie. Houten: Bohn Stafleu van Loghum.